Complex SABR for all
Long term follow up data from studies such as the SABR-COMET Trial and improved access to these treatments nationally mean that SABR is now considered a standard of care for the management of oligometastatic disease.
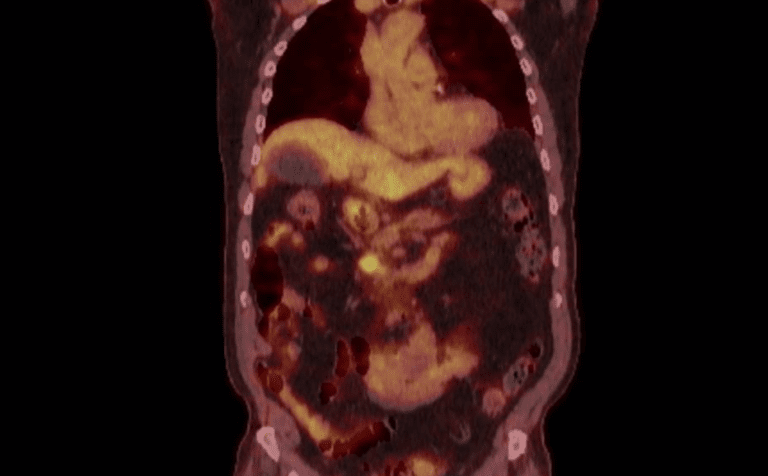
I recently met an 81 year old gentleman who had had a right radical nephrectomy in 2014 for a pT1b Nx M0 Grade 2 clear cell renal cell carcinoma. He had been treated and followed up in the NHS and was found to have an incidental 16mm hyper vascular lesion in the pancreatic head on his five year surveillance CT scan, which had been delayed slightly due to the Covid-19 pandemic. With no other abnormalities identified, and a performance status of zero he had been referred to the upper GI team for further investigation and when biopsied this was confirmed to be a metastasis from his previous renal cell carcinoma, now 6 years since his original diagnosis and surgery. He came to see me in my private clinic to discuss his potential treatment options and I requested a PET CT scan which showed this to be a solitary site of disease.
Fig 1: Fused coronal PET CT image showing pancreatic metastasis.
Given the insidious nature of this disease I knew immediately that I should consider potentially curative focal treatment. Being a pancreatic lesion, this type of complex SABR treatment is currently outside of my expertise, yet working with GenesisCare I am able to access this state-of-the-art treatment for my patients.
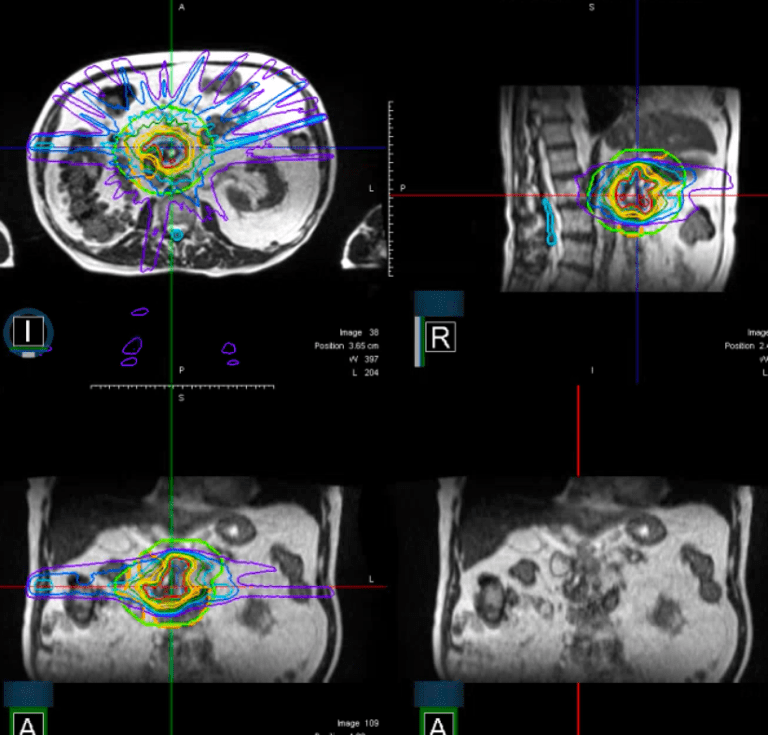
In addition, my work on the MRIdian MR-linac in Oxford has shown me first-hand the greatly improved soft tissue definition achievable on this machine. For a pancreatic lesion sitting adjacent to the duodenum this improved definition becomes invaluable, together with the ability to review and edit the target and the organs at risk for each fraction. It is then possible to reoptimize the plan for the daily anatomy, before treating the patient whilst tracking the tumour and gating the dose delivery. All of this increasing the likelihood of delivering truly ablative doses to the target, whilst reducing the volume of normal tissue being irradiated.
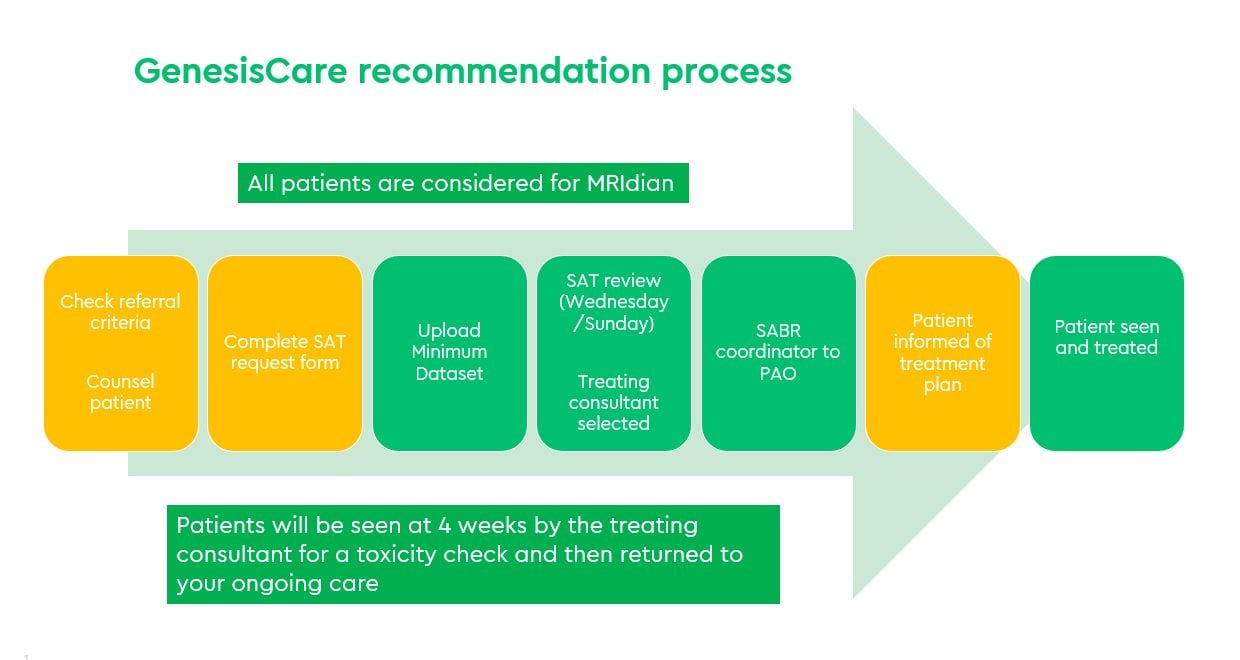
For my patient, I completed a SABR Advisory Team (SAT) proforma and supplied the required clinical data set. Two days later I received the review outcome accepting my patient for treatment and within two weeks he had met the treating oncologist and attended for treatment planning. He has subsequently been planned to receive 40 Gy in 5 fractions treating on alternate days. The plan has achieved all the OAR constraints and as I write he is part way through his treatment course and tolerating it well.
Fig 2: MRL plan
At GenesisCare all potential SABR patients are reviewed by the SABR Advisory Team (SAT) in the twice-weekly virtual SAT MDT. SAT comprises of a multi-disciplinary team of doctors specialising in the relevant tumour areas. For simple SABR (peripheral lung lesions, non-spine bone metastases and pelvic lymph node metastases), a credentialling programme with peer review of cases is available for all consultants practising at GenesisCare, enabling them to offer local simple SABR treatments to their patients which in turn supports the National roll out of simple SABR within the public sector.
Complex SABR treatments (liver, spine, pancreas, central lung lesions and reirradiation) is also available to all GenesisCare Consultants and their patients. If a consultant does not have prior demonstrable experience, they can recommend patients via the SABR Advisory Team who will allocate a credentialed Oncologist, and where appropriate patients can be treated on the MRIdian MR-linac at GenesisCare in Oxford.
If you would like more information about how to access these treatments for your patients, please don’t hesitate to contact sabr@genesiscare.co.uk
Dr Nicola Dallas
Clinical Oncologist
MBChB, MRCP, FRCR




