GenesisCare pushing the boundaries with MR Linac SABR
Since the Covid19 pandemic struck in March, surgical services for cancer patients have been near paralysed, and many centres have had to cutback on both systemic therapy and radiotherapy due to resource issues and patient safety. Stereotactic radiotherapy enables ablative doses of radiation to be delivered to patients non invasively and with minimal hospital visits in a covid free environment; for patients with oligometastatic disease (1 – 5 metastases) studies have shown impressive survival and ablation rates similar to RFA and some surgical series. GenesisCare has advanced SABR platform technologies and a group of highly skilled dedicated clinicians able to perform ablative radiotherapy treatment to cancer patients.
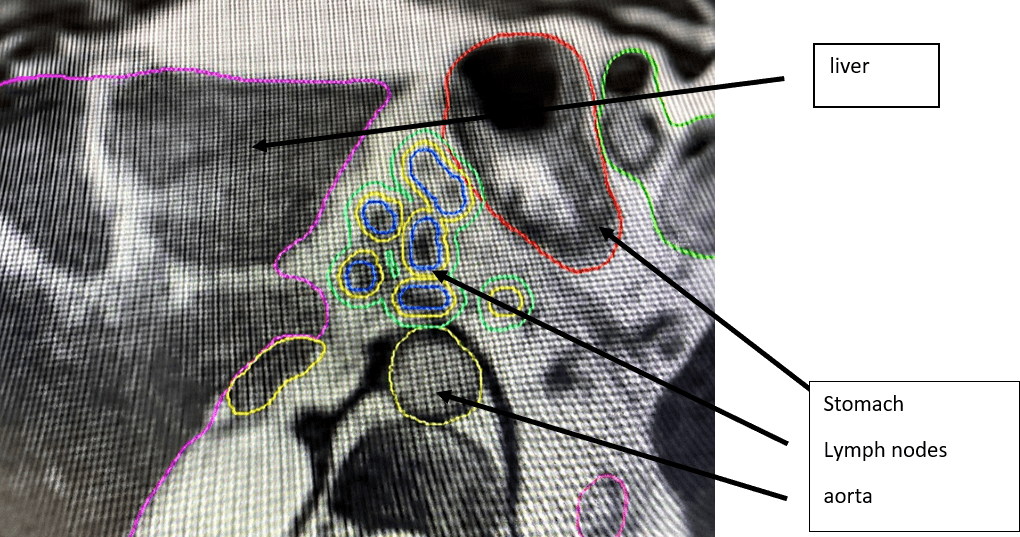
We illustrate the case of a fit male in his mid 60’s previously treated with surgery and adjuvant chemotherapy for a HER2+ MSI Stable colon cancer, who relapsed with nodal disease above and below the diaphragm. A few months following complete radiological and metabolic response of his nodal disease to further chemotherapy he developed oligoprogression in a small nodal cluster around the coeliac axis (see pic). This was not amenable to surgical resection. Stereotactic radiotherapy was recommended to the site of oligoprogression. Cyberknife was declined due to the risks associated with fiducial marker insertion in this location. Conventional non gated linac SABR would be possible but dose would have to be restricted significantly to meet organ at risk tolerance. Due to the proximity of normal tissues, daily variations in stomach and bowel position, and significant respiratory motion, MR Linac guided SABR was recommended. With automatic respiratory gating, daily recontouring of target and organs at risk, and adaptive replanning and reoptimisation a potentially ablative dose of 40Gy in 5 fractions was achieved. Treatment was very well tolerated with nausea and fatigue very manageable. Without MRL, one would have to question the value of “low” dose SABR in this location. This patient was treated with confidence and as a result has been able to stay off systemic therapy for significantly longer, thus improving quality of life. Early results from the SABR-COMET trial also suggest that SABR to oligometastatic disease improves survival over and above standard of care – 42% vs 17% 5 year overall survival.