
Multiple spinal metastases
Dr John Conibear
Dr Conibear is currently deputy medical director and deputy director of Barts Cancer Centre. He specialises in all the non-surgical treatments for both lung and breast cancers.

Case presentation
In December 2021, a 59-year-old woman presented with a short history of pain in her neck radiating down both arms. She had a past medical history of both early triple negative breast cancer (2007) and early rectal cancer (2019).
Challenges of presentation and choice of treatment
Investigations, including an MRI scan of her spine, revealed multiple bone metastases in her spine, C7, T1 and T3. Her PET-CT confirmed metabolic uptake in her bone metastases plus multiple small lung nodules.
In January 2022 she underwent neurosurgical decompression of C7 with plate fixation and the post-operative histology confirmed metastatic colorectal cancer. She was then referred for SABR to the post-operative bed, C7 - T1, and T3 vertebral metastasis.
Spine SABR treatment
In February 2022, she received SABR to C7-T1 and T3. A total dose of 30Gy in 5# on alternate days was delivered using a Varian Edge Linac. She tolerated the treatment will without any significant acute toxicities.
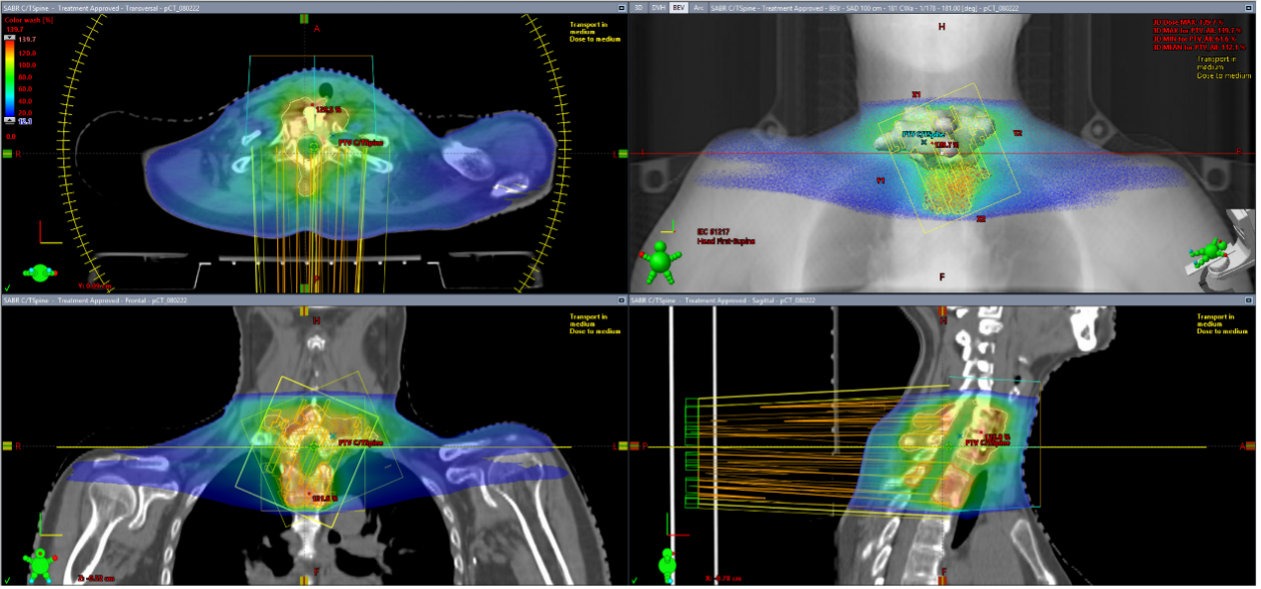
Figure 2: Treatment planning on Varian Edge Linac
Results and follow-up
In May 2022, approximately 3-months since finishing her SABR, she had complete resolution of her back pain. In May 2022 she underwent a post-treatment PET-CT scan which revealed a complete metabolic response of her T3 vertebral metastasis, and persistent although reduced tracer uptake relating to the anterior stabilisation of C6-T1 vertebra. The patient now continues on active surveillance.
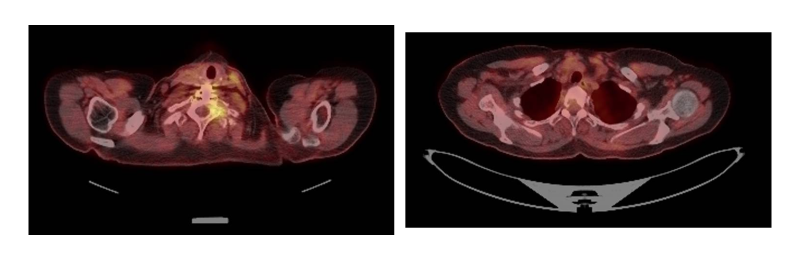
Figure 3: Post-SABR PET-CT
For more information or to refer a patient contact us at sabr@genesiscare.co.uk
Solitary spine metastases
Dr John Conibear
Dr Conibear is currently deputy medical director and deputy director of Barts Cancer Centre. He specialises in all the non-surgical treatments for both lung and breast cancers.
Case presentation
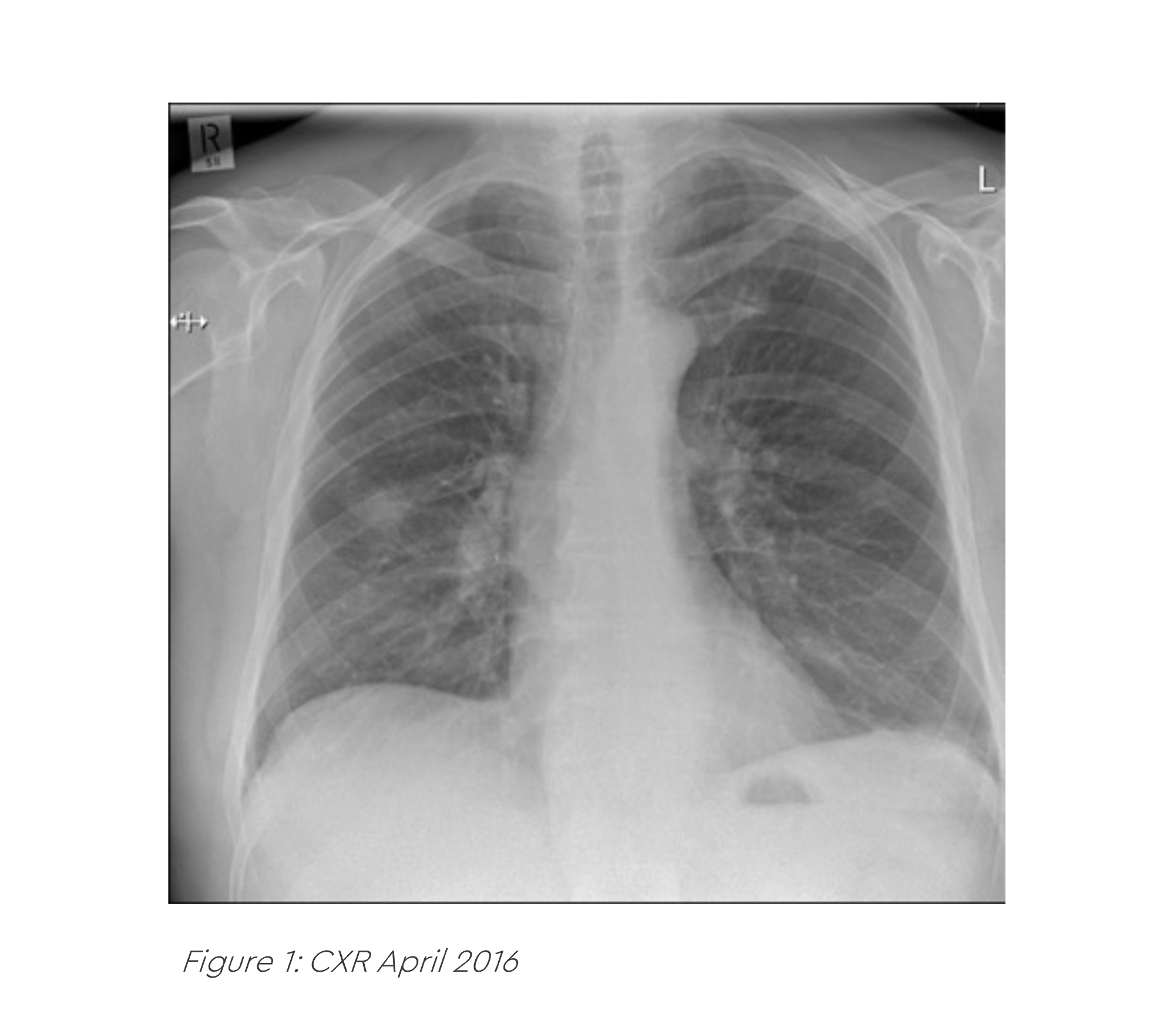
A 64-year-old gentleman presented to his GP in February 2016 with a persistent cough and new onset back pain. He was prescribed multiple courses of oral antibiotics, but his symptoms did not settle and a subsequent CXR in April 2016 was reported as abnormal. He was referred on a 2WW pathway to his local hospital where he had an urgent CT of his chest. This revealed a right lung mass, enlarged right hilar lymph nodes and a lytic metastasis in his T7 vertebra.
An EBUS was undertaken which confirmed an adenocarcinoma of the right lung. It was EGFR mutation negative and ALK fusion negative. A PET-CT scan confirmed his stage was T1b N1 M1b (solitary T7 met). An MRI scan of his brain was normal.
Challenges of presentation and choice of treatment
In May 2016 he commenced monthly Denosumab plus pemetrexed and cisplatin chemotherapy. In July 2016 he completed four cycles of pemetrexed and cisplatin chemotherapy and then commenced maintenance pemetrexed in August 2016. His repeat PET-CT in July 2016 showed an excellent response to treatment with a complete metabolic response in all sites of disease initially identified.
He was therefore referred for a right VATS lobectomy and nodal dissection 12th October 2016. Post operative histology revealed a small amount of residual tumour in the primary specimen but no viable tumour in the right hilar lymph nodes. The post-operative stage was ypT1b ypN0 M1 R0.0.
Spine SABR treatment
Following surgery, the patient was referred for consolidation SABR to his T7 vertebral metastasis which he completed on the 2nd of December 2016. A total dose of 24 Gy in 3 fractions on alternate days was delivered.
Results and follow-up
The patient experienced no significant acute side effects and recommenced maintenance Pemetrexed and Denosumab. In November 2016, his maintenance Pemetrexed was ceased and in January 2018 his monthly Denosumab was ceased. As of May 2022, 75 months since his original diagnosis, the patient remains disease free with no signs of active disease on imaging. He continues active surveillance and remains performance status 0 with no long-term toxicities.
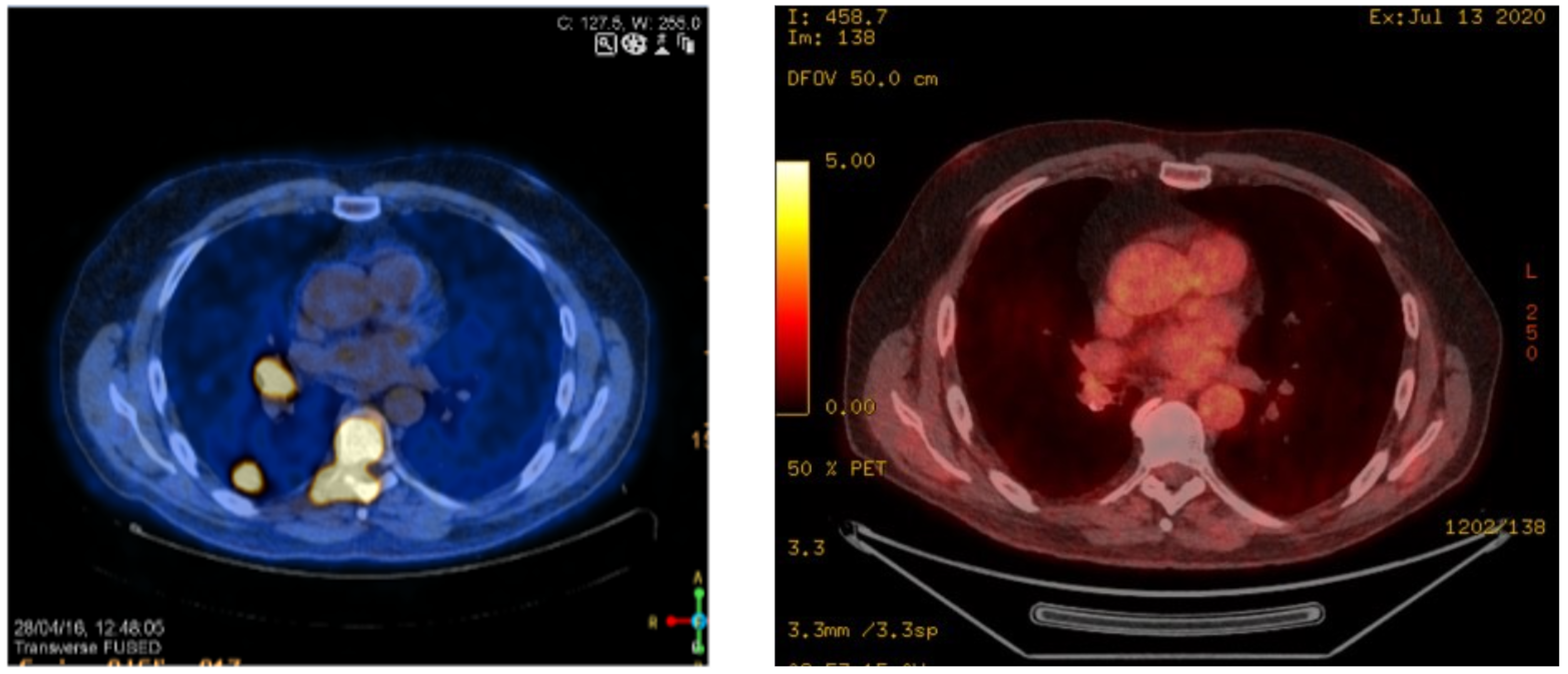
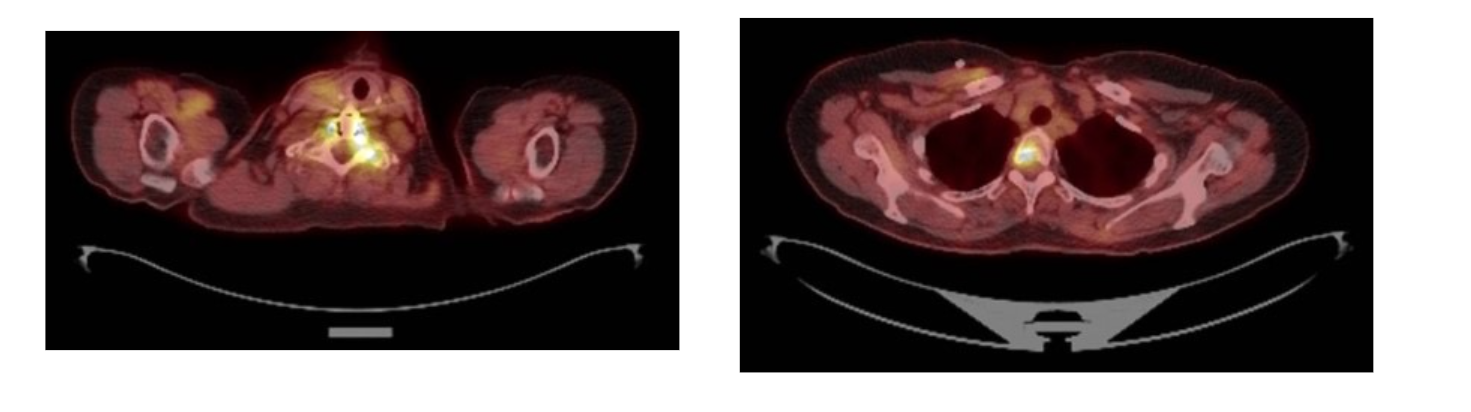
Figure 2: NM PET Scan April 2016
Figure 3: FDG PET Scan May 2022
For more information or to refer a patient contact us at sabr@genesiscare.co.uk
2# SABR to painful spinal metastases
Dr Luis Aznar-García
Dr Luis Aznar-Garcia is as a Consultant Clinical Oncologist and is involved in Stereotactic ablative radiotherapy (SABR/SBRT) for Oligometastases, Hepatobilliary (HpB) tumours, breast cancer and the use of SRS for brain tumours.

Case presentation
A 54-year-old lady with metastatic breast cancer presented with lumbar pain from an L3 metastasis in July 2022.
The patient was initially diagnosed in 2007 and received surgery, followed by chemotherapy and radiotherapy. 10 years later she presented with lung metastases and a painful metastasis in the left scapula, which was treated with radiotherapy (8 Gy in one fraction). She started treatment with Palbociclib, Denosumab and endocrine therapy
By the next presentation of lumbar pain in July 2022, Capecitabine was added to her systemic treatments. A whole spine MRI showed L3 metastasis at the level of her new lumbar pain.
Challenges of presentation and choice of treatment
The patient was offered 8 Gy in one fraction or 20 Gy in five fractions on the NHS, but made an appointment with her Clinical Oncologist Consultant, Dr Luis Aznar-García, at GenesisCare for a second opinion. Having reviewed her case and MRI scan, the patient was advised that SABR treatment, based on evidence from a randomised clinical, has shown better pain control with a SABR treatment of 24 Gy in two fractions than palliative conventional radiotherapy at three and six months.
This evidence is based on the phase III CCTG SC.24/TROG 17.06 trial1 from the Canadian Cancer Trials Group which compared SABR (24 Gy in two fractions) to conventional radiotherapy (20 Gy in five fractions) in patients whose primary tumours had metastasised to painful spinal lesions. Here, 35% of patients in the SABR arm reported a complete pain reduction at three months versus 14% from the conventional radiotherapy arm. This remained consistent at six months, with complete response rates of 32% and 16%, respectively.
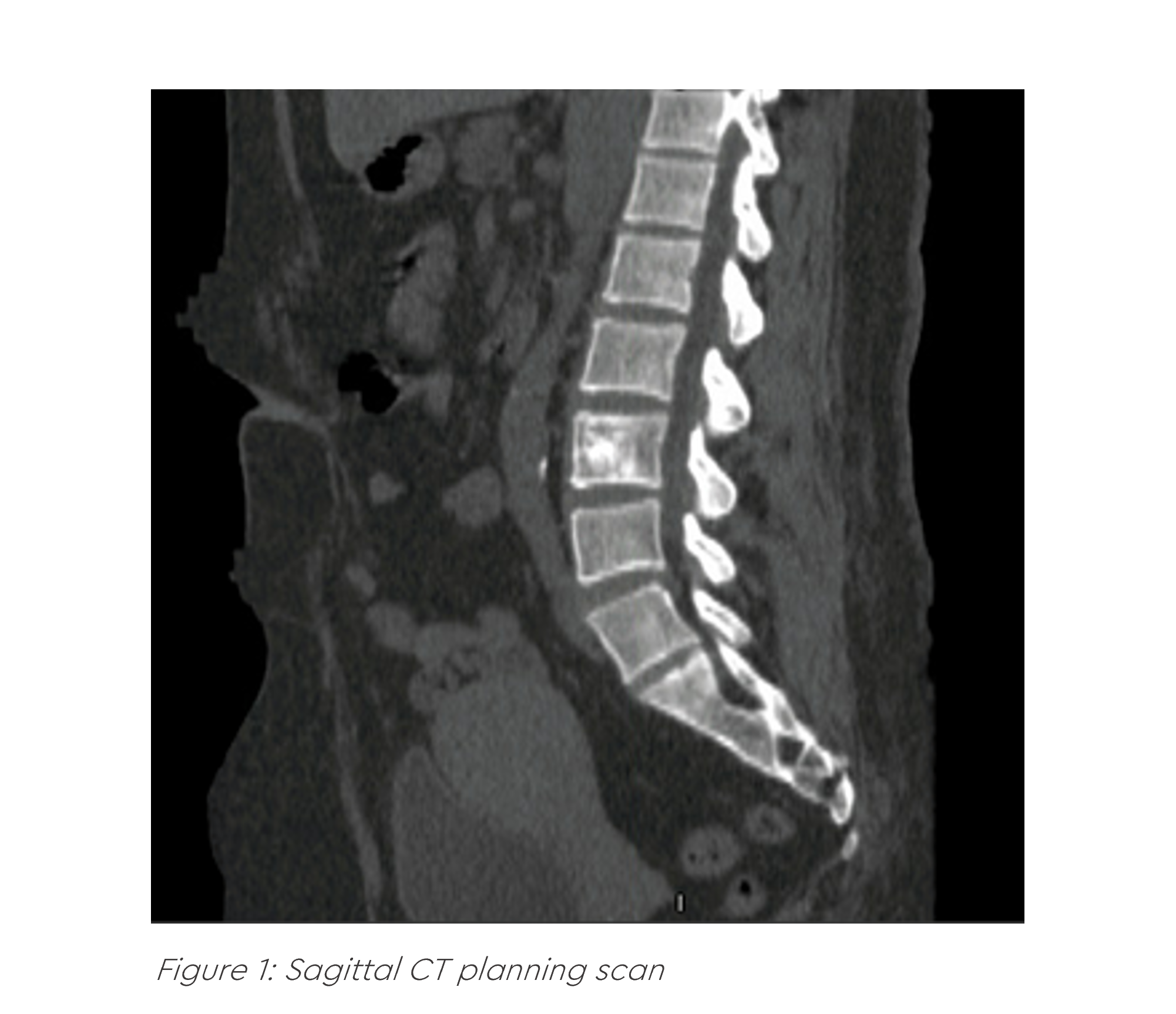
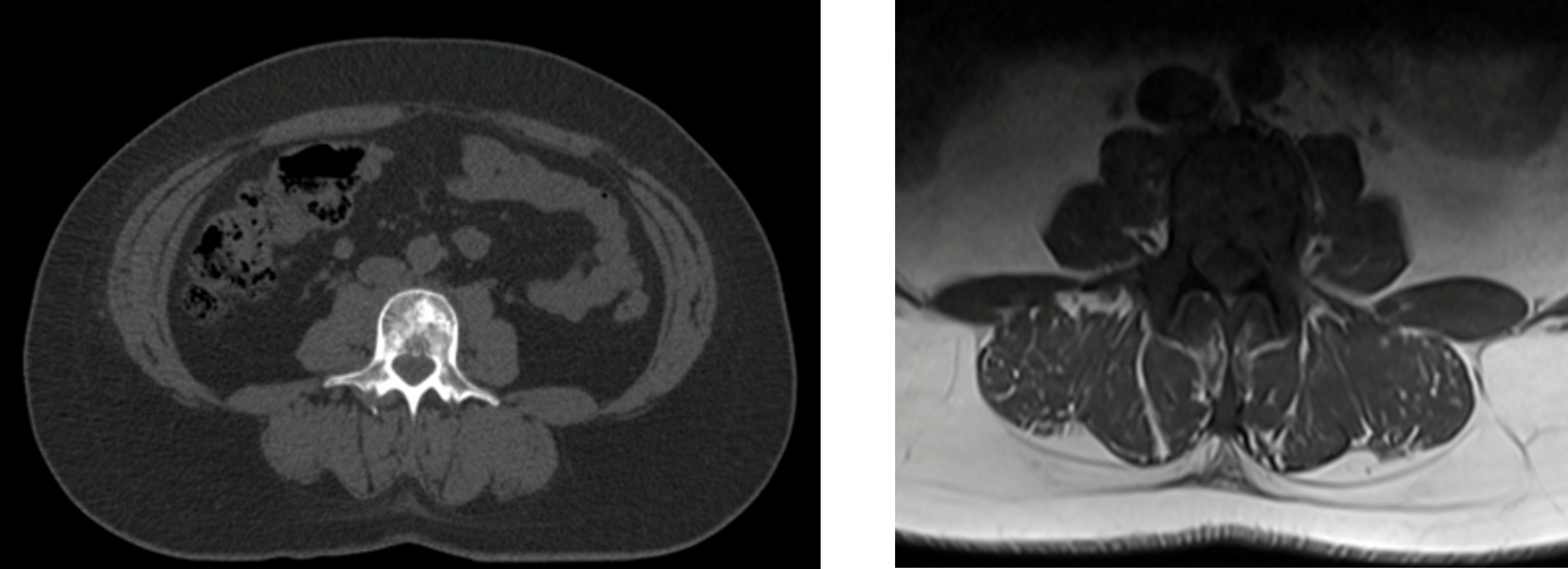
Figure 2: Axial CT planning scan
Figure 3: Axial MRI planning scan
The case was referred for discussion to the SABR Advisory Team and it was decided the patient was suitable for SABR to spinal metastases to control pain at GenesisCare Oxford. The patient was otherwise healthy with no comorbidities.
SABR treatment
The aim of treatment was to ablate the L3 metastasis and provide optimal pain control. The patient received 24 Gy in two fractions to the L3 metastasis. Treatment was given on alternate days with the patient spending 30–40 minutes on the table, less than the average 45 minutes due to the patient’s fitness level.
Results and follow-up
At three months post-treatment with SABR, the patient experienced a significant improvement in her quality of life. Her pain score decreased from 8/10 to 1/10, while performance status improved from 2 to 0–1. Previously unable to leave the house, the patient is now able to go for long walks with her husband without having pain and is off pain medication.
Discussion
Randomised evidence shows that SABR offers better and more durable pain control than conventional palliative radiotherapy.
Reference
- Sahgal A, Myrehaug SD, Siva S, Masucci L, Foote MC, Brundage M, et al. CCTG SC.24/trog 17.06: A randomized phase II/III study comparing 24gy in 2 stereotactic body radiotherapy (SBRT) fractions versus 20gy in 5 conventional palliative radiotherapy (CRT) fractions for patients with painful spinal metastases. International Journal of Radiation Oncology*Biology*Physics. 2020;108(5):1397–8.
For more information or to refer a patient contact us at sabr@genesiscare.co.uk

You are leaving our website
You are now leaving our website. GenesisCare do not control this content and therefore are not responsible for its accuracy or reliability.