
Spine Reirradiation: Advances in Stereotactic Radiotherapy
Stereotactic radiotherapy (SABR) to the spine is established as a safe and effective treatment in several clinical scenarios. Spine SABR can be used to treat oligometastatic disease1 and also to palliate symptomatic vertebral metastases2. As a result, spine SABR is now recommended in a number of national and international guidelines3,4,5.
Due to improvements in the effectiveness of surgery, radiotherapy and systemic therapy, it is becoming increasingly common that patients will receive multiple lines of anti-cancer therapy. This brings new challenges to treating clinicians, and Clinical Oncologists are increasingly likely to need to consider and manage the complexities of reirradiation.
Stereotactic radiotherapy to the spine is usually delivered as a second or subsequent line of therapy. As a result, in some patients there will be overlap between a prior course of radiotherapy and the target for spine SABR. Examples could include a patient who has previously received radical radiotherapy for laryngeal cancer and now requires stereotactic radiotherapy to an oligometastatic cervical vertebral metastasis, or a patient who has a painful vertebral metastasis but who has already received stereotactic radiotherapy to the adjacent vertebral body.
An overarching concern in the reirradiation setting is how cumulative doses to organs at risk translate into the risk of late radiation toxicity for the patient. This is particularly important in the context of spine reirradiation given the critical organs at risk in the region of interest, such as the spinal cord and cauda equina.
Dose contribution from a previous course of radiotherapy to a specific segment of the spinal cord is no longer an absolute contraindication to future spine SABR to the same region. Close collaboration between clinicians and the radiotherapy planning team, taking into account previous radiotherapy dose and working to agreed clinical protocols, means that it is often possible to produce a safe and deliverable spine SABR plan which delivers a higher dose of radiotherapy to the tumour than could be achieved with conventional radiotherapy.
Clinical case study
As an example, a 67 year old patient received radical chemoradiotherapy for stage III adenocarcinoma of the left upper lobe. Two years later he developed oligometastatic disease in the T7 and T8 vertebral bodies which was treated with stereotactic radiotherapy. After a further four year interval the patient developed a painful metastasis within the T9 vertebral body. The treating clinician wanted to offer the patient stereotactic radiotherapy to the T9 metastasis because of the improved pain response compared to conventional radiotherapy, however the two previous courses of radiotherapy contributed dose to the area which now required further treatment.
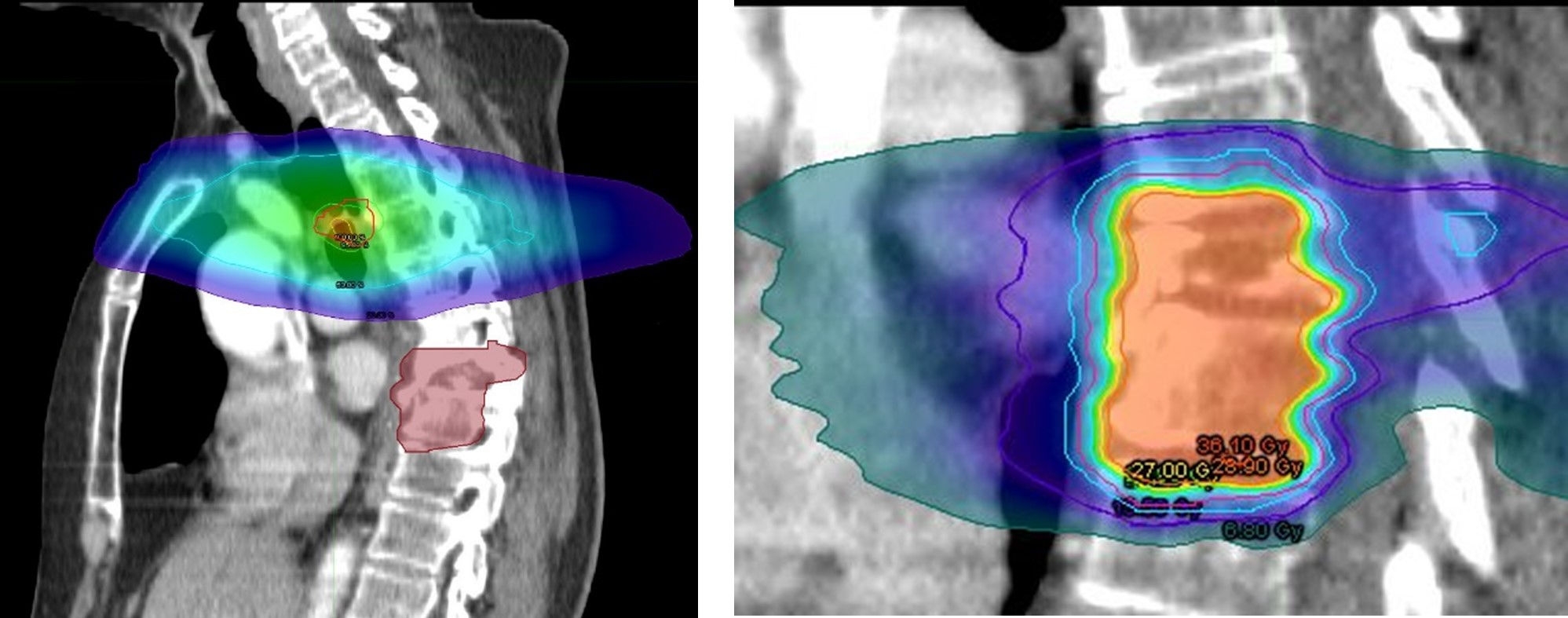
Figure 1: The previous courses of lung radiotherapy and spine SABR both contributed dose to the spinal cord in the region where further spine SABR was planned.
The radiotherapy planning team were able to model the previous treatments on a new radiotherapy planning scan and then calculate the remaining tolerance to each level of the spinal cord. A SABR plan was then created which respected the remaining tolerance of the cord. PTV coverage was compromised to achieve the bespoke spinal cord constraints, but the spinal SABR plan was delivered safely resulting in a higher dose to the tumour than could have been achieved with conventional radiotherapy.
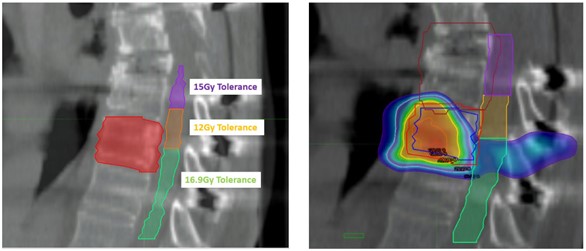
Figure 2: It was possible to produce a safe spinal SABR plan to treat the T9 vertebral metastasis whilst respecting bespoke cord tolerance constraints
Given that spine SABR and spinal reirradiation cases are often complex, the GenesisCare SABR MDT is supported by a Consultant Spinal Surgeon. Referring clinicians receive an opinion on the suitability for spine SABR via the MDT outcome, which also includes a spinal surgical opinion regarding spinal stability and the suitability for separation surgery.
Conclusion
In summary, stereotactic radiotherapy to the spine can be considered even if the spinal cord in that area has received radiotherapy dose previously. The experienced radiotherapy planning team and clinicians in the Stereotactic Radiotherapy Clinical Reference group would be happy to discuss cases and support referring clinicians wherever possible.
Refer today
To refer to one of our specialists or to find out how we can help you and your patients, contact us at the below email.
Dr Peter Dickinson
Consultant Clinical Oncologist
GenesisCare UK
References
1. Palma, David A et al. Stereotactic ablative radiotherapy versus standard of care palliative treatment in patients with oligometastatic cancers (SABR-COMET): a randomised, phase 2, open-label trial The Lancet, Volume 393, Issue 10185, 2051 – 2058
2. Sahgal A et al, A Randomized Phase II/III Study Comparing 24Gy in 2 Stereotactic Body Radiotherapy (SBRT) Fractions Versus 20Gy in 5 Conventional Palliative Radiotherapy (CRT) Fractions for Patients with Painful Spinal Metastases. Int J Radiat Oncol Biol Phys. 2020 Dec 1;108(5):1397-1398
3. UK SABR consortium guidelines. Accessed June 2025. https://www.sabr.org.uk/wp-content/uploads/2019/04/SABRconsortium-guidelines-2019-v6.1.0.pdf
4. NICE Spinal mesastases and metastatic spinal cord compression guideline. NG234. Accessed June 2025 https://www.nice.org.uk/guidance/ng234
5. Guckenberger, M et al. ESTRO clinical practice guideline: Stereotactic body radiotherapy for spine metastases. Radiotherapy and Oncology, Volume 190, 10996
